“For 17 Years I Watched Patients Sleep With Their Feet Off The Mattress. Their Nerve Tests Were 'Clean.' Then I Found The Compound No Discharge Note Has Ever Named.”
By the second week, sleep comes back. Six months later, my patients are still in their own bed.Here is exactly what I found, in the order I found it.


If your feet catch fire the moment you lie down.
If your nerve test came back "clean."
If three specialists already told you it is your age.
It took me 17 years and roughly 400 patients to learn what the discharge note is missing.
The 2am burning is not a sleep problem.
It is a small-fiber nerve firing a false alarm.
The compound your body makes to quiet that nerve is called PEA.
Production runs short under sustained stress. The standard workup is not built to see it.
Not one patient who counted their sleepless nights in my office had ever been told this compound existed.
Not in the nine-minute appointment. Not in fourteen months of discharge notes.
By the second week, sleep was often the first thing that came back.
The first sensory change sometimes started inside the first week: less 2am burning, less feet-off-mattress bargaining, one uninterrupted stretch of sleep.
Six months later, the patients who responded were back in their own bed and had forgotten to be amazed by it.
This is not magic and it is not fast for everyone. A minority of people in the trials saw no meaningful change. I am going to tell you exactly what I found, in the order I found it.
Dr. Helen's Case Notes

Eleanor was sixty-three.
Her nerve test came back clean.
Her circulation was fine.
Three specialists had told her the fire in her feet at 2am was just her age.
A year earlier she was walking three miles every morning.
Now she slept with her feet hanging off the end of the bed.
She could not stand the weight of a sheet on them.
"They look at the tests, tell me there's nothing there, and send me home," she said.
"They think I'm making it up."
She was not making it up.
291 Nights: The Phone Log A Retired Teacher Showed Me
A man came in last month. Sixty-seven. Retired teacher.
He had not slept a full night in fourteen months.
He had it written in his phone.
Two hundred and ninety-one nights.
His wife had started sleeping in the other room.
Not because of him, he said quickly. His pacing at 3am kept waking her.
He said that part looking at the floor.
That is the cost no test measures.
Not the pain score.
The slow narrowing of a life down to the hours between lying down and giving up.
Ninety Minutes For One Sentence: "Likely Age-Related"
By the time someone reaches me, they arrive with a history I could almost recite.
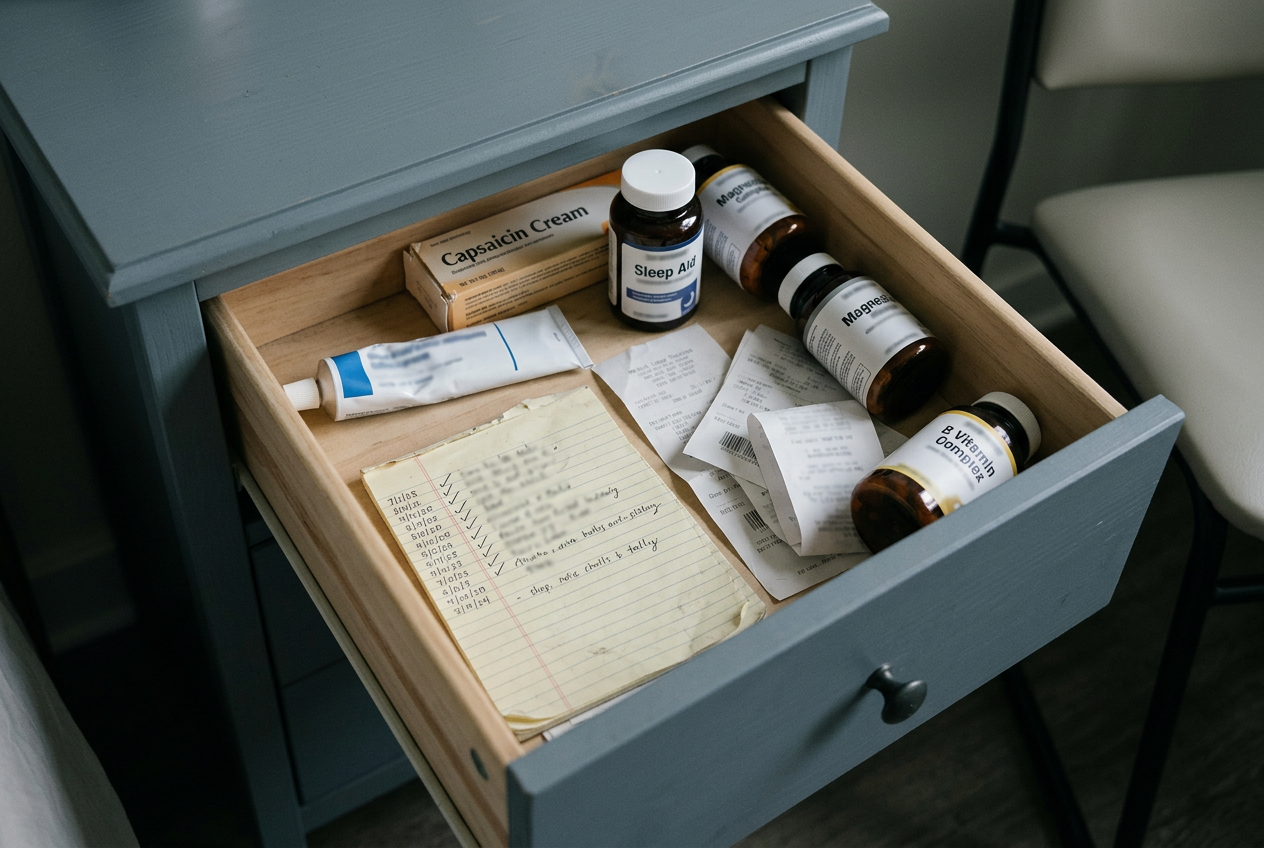
Lidocaine cream from the first doctor. The surface was never the problem.
Capsaicin cream from the second. Usually made it worse.
An over-the-counter sleep aid. A drawer of magnesium and B vitamins.
For some, gabapentin. They describe it the same way every time: trading the fire for a fog.
The retired teacher brought me his neurology discharge note.
It said, in full:
"Likely age-related. Reassured patient. Recommended topical lidocaine PRN."
He had driven ninety minutes each way for that sentence.
I set the note down.
The appointment had been built to end, not to find anything.
Most of the people who write those notes are not villains. They have nine minutes and a full waiting room.
The object on the patient's nightstand is identical either way. A tube that was never going to reach the nerve.
By my rough accounting, the average patient who reaches me has already spent north of four hundred dollars on creams, sleep aids, and copays.
Plus a year, sometimes two, of nights they will not get back.
One ordinary Thursday I caught myself writing "likely age-related" in my own notes.
I put the pen down.
I was done writing a sentence I no longer believed.
So I started pulling the actual research. The double-blind trials. Not the summaries.
The compound had been studied for years.
The data had been sitting there the whole time.
And not one of the men and women who counted their sleepless nights in my office had ever been told it existed.
Why The Fire Waits Until 2am
Feet bearable through the day.
The moment they lie down, the burning starts.
They have been told it is insomnia. It is stress. The room finally went quiet.
It is none of those.
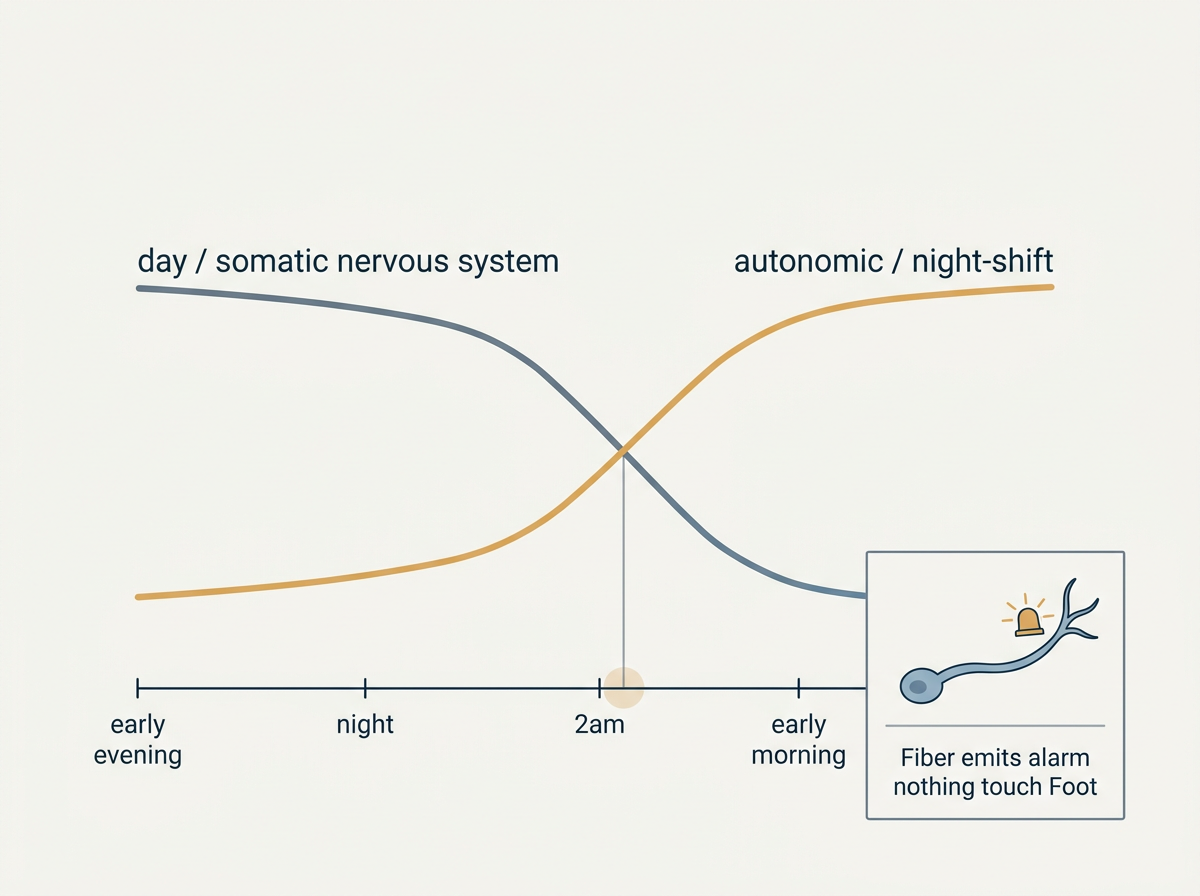
When you lie down, the day part of your nervous system powers down.
A second system takes the night shift. The autonomic nervous system.
In a small-fiber nerve injury, it does not idle quietly. It amps up.
The fire is not worse at 2am because the house is quiet.
It is worse at 2am because that is the shift when the damaged wiring is in charge.
The nerve sends a pain signal when nothing at all is touching the foot.
A detector going off in a room with no smoke in it.
Painkillers numb your whole body to mute the noise.
PEA is the compound your body already makes to quiet the one nerve that's on fire.
PEA is not a drug.
It is a fatty compound your own body manufactures to calm exactly this kind of over-firing.
Production runs short under sustained nerve stress.
Supplying more of it does not sedate you. It does not deaden the foot.
It works on the cell that is doing the screaming.
The shelf gets it wrong in two ways. Most products get both.
One: PEA is barely absorbed in its raw form. It has to be milled fine (what the label calls micronized) or your gut passes most of it unused.
Two: the trials used 600mg a day. Below that, you have swallowed a capsule your body cannot use.
This is also why every cream failed.
A cream treats the surface. The fire was never on the surface.
A sleep aid sedates the brain. The brain was never the broken part.
Both aim at the smoke. Neither reaches the detector.
What I Started Putting In Front Of Them
I do not sell anything.
I have no arrangement with the company whose bottle I am about to name.
I went into this looking for a reason not to trust it.
What I found was the version that matched the research instead of the marketing.

Check the form: micronized, milled fine enough to absorb.
Check the dose: 600mg, the studied amount, not a smaller number dressed up as nerve support.
It is sold as Youfirst PEA.
Aggregate review of multiple clinical trials. Verified independently before launch.
I began pointing patients to it the same way I would point them to any dose I had read the trials on.
Then I did the only thing that means anything in a clinic.
I watched what happened.
The sleep came back before the pain did.
Almost every time. Patients arrived surprised, telling me they had slept the whole way through for the first time in months.
Sleep is the first thing PEA tends to give back, ahead of the pain itself. The trial that anchored all of this reported the same order of events.
The pain scores moved next. Slowly. Not to zero.
The honest number, in my chairs, is a burning that goes from running the entire night to a low hum they forget to mention.
Walter was the retired teacher with the discharge note and the ninety-minute drive.
I gave him the same caution I give everyone. It is not fast. Sleep tends to come first.
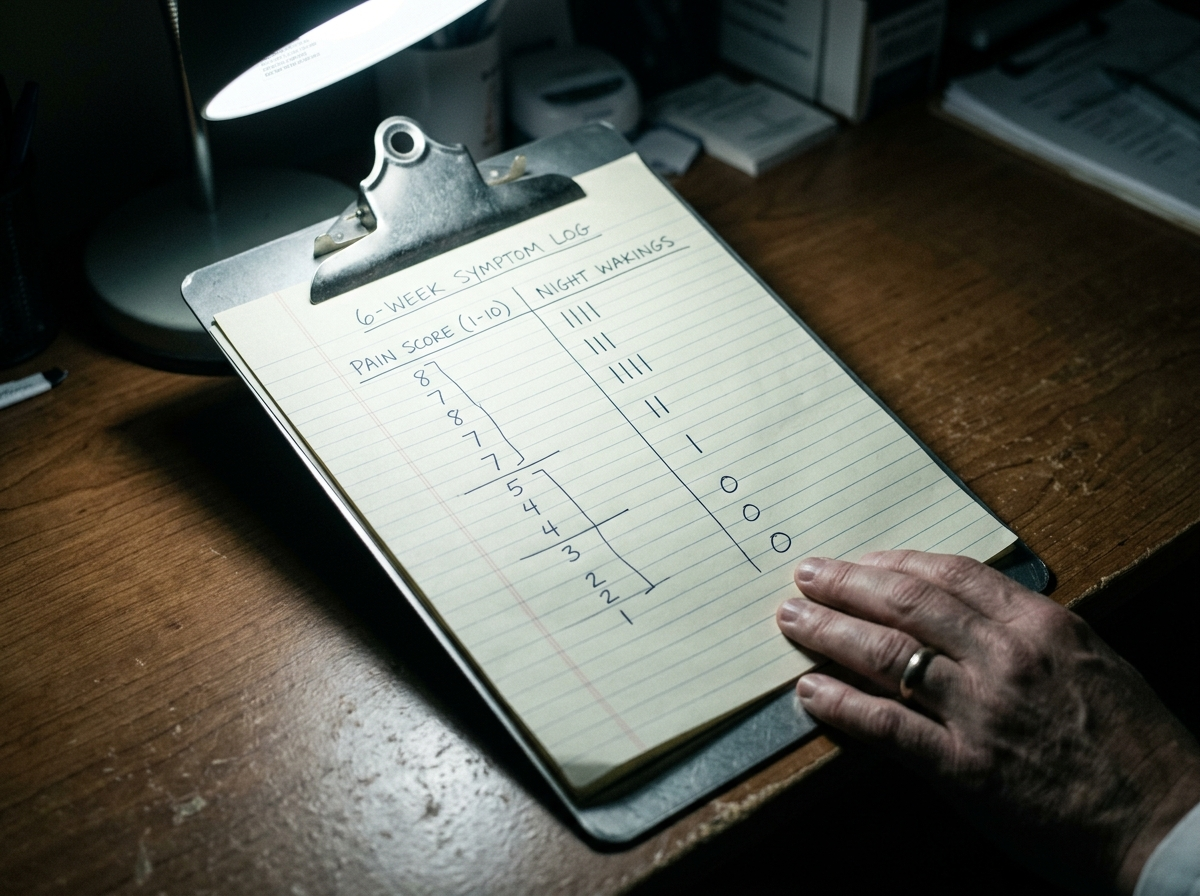
Here is what his own log looked like by week six.
| Measure | At intake | By week six |
|---|---|---|
| Burning at lights-out (0–10) | 8 | 2 |
| Nights waking from foot pain (per week) | 7 | 1 |
| Could tolerate a sheet on the feet | No | Yes |
| Sleeping in his own bed | No | Yes |
He ran his own version of the test the skeptics always ask me for.
He stopped taking it for a stretch.
By the fifth night the count started climbing again.
He called the office, a little sheepish, and told me he would not be running that experiment a second time.
The pause test is the only proof I actually trust. The patient runs it on himself and there is no one there to sell him the result.
The $400 Cabinet Versus A Dollar A Day
When a patient asks me what it costs, I tell them to first add up what the last two years already cost.
It lands harder than anything I could say.
| What they already tried | Roughly |
|---|---|
| Creams and topicals (lidocaine, capsaicin, the rest) | $120 |
| Sleep aids and supplements that missed the cause | $110 |
| Specialist copays for appointments that ended in a cream | $180 |
| Spent before anything reached the nerve | north of $400 |
Against that, the compound that actually reached the nerve runs about a dollar a day on the subscription. Less on the buy-two-get-one.
If you change nothing, I can tell you with some confidence how tonight goes, and the night after that.
What another year of this actually costs you.
- The night cost: 365 more nights, often 2 to 3 pain alarms each night. That is 730 to 1,095 chances to wake up and bargain with your own feet.
- The money cost: another $400 cabinet can become $800 or more once the creams, sleep aids, copays, and new bottles repeat themselves.
- The health-risk cost: chronic pain plus broken sleep tends to widen the risk categories patients already fear, falls, mood strain, medication escalation, and lower daily movement.
- The relationship cost: the separate bedroom, the pacing at 3am, the spouse who learns to sleep around your pain instead of beside you.
- The nerve cost: the wire does not heal itself just because you learn to live around it.
I am a podiatric physician who has spent 17 years listening to people describe burning feet. One patient phrase has never left me: "I waited 4 years before I tried this. I cannot get those 4 years back."
That is the line I think of when someone tells me they can probably tolerate one more year.
The thing that makes this defensible to me is the 90-day money-back guarantee.
That is the company letting you run the pause test on their own dime.
I have never once seen a tube of cream make that offer.
Do the thing almost none of my patients were given the chance to do at the start.
Read the dose and the form for yourself. If it matches what the trials used, give it the weeks it needs.
What the offer actually says
- Subscription: one bottle for $29.99.
- Subscription Buy 2 Get 1 Free: $59.99.
- One-time: one bottle for $39.99.
- One-time Buy 2 Get 1 Free: $79.99.
Ninety days, and if it does nothing for you, you send it back for your money.




P.S.
Walter came in last month for a callus.
On his way out he mentioned his wife had been back in their own bed for half a year, and that he had forgotten to be amazed by it.
That is the outcome I was never able to write on a discharge note.
It does not fit on the line where they print "reassured patient."
If the current batch of 1,384 bottles is gone, it is usually weeks before the next one is milled, tested, and released.