“I'm A Podiatrist. For 17 Years I Watched Burning-Feet Patients Spend $400 On Creams That Couldn't Reach The Layer That Was On Fire.”
By week two, the sheet was back over her feet. By month two, she was walking her dog the old two miles. Here's what I now hand the patients who tried everything.


If you're reading this because your feet catch fire the second they touch the sheets, here's what it took me seventeen years of podiatric practice and one Tuesday afternoon with a woman emptying her bag of creams onto my exam paper to understand.
The fire was never on her skin.
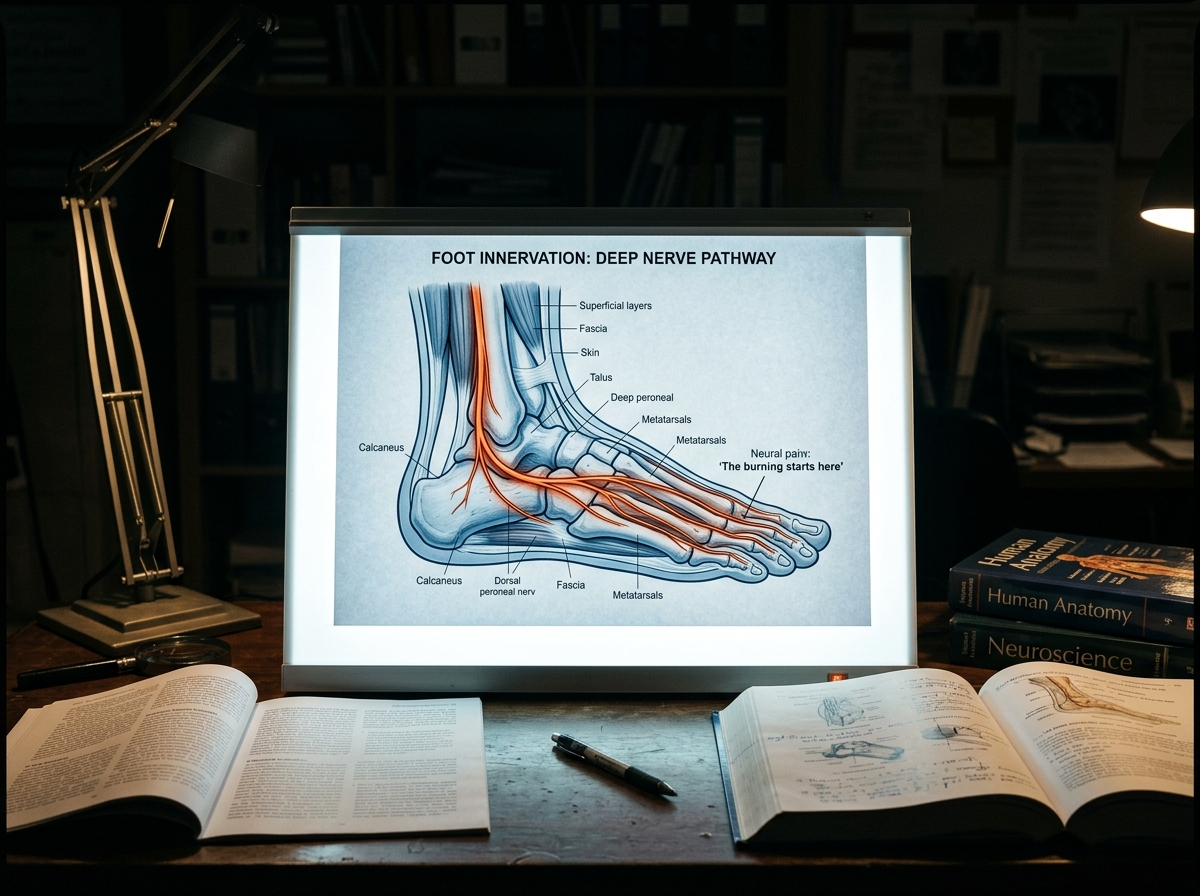
The burning is coming from the small nerve fibers just beneath it, misfiring, reporting a fire that is not there.
Every cream in that bag was aimed at the surface. The wire was always one layer below the depth they reach.
What finally quiets the wire is a compound the body already makes, called PEA, milled small enough to absorb (micronized), at the 600mg the published trials used.
No referring physician I ever called had named it.
Not in a chart note. Not in seventeen years.
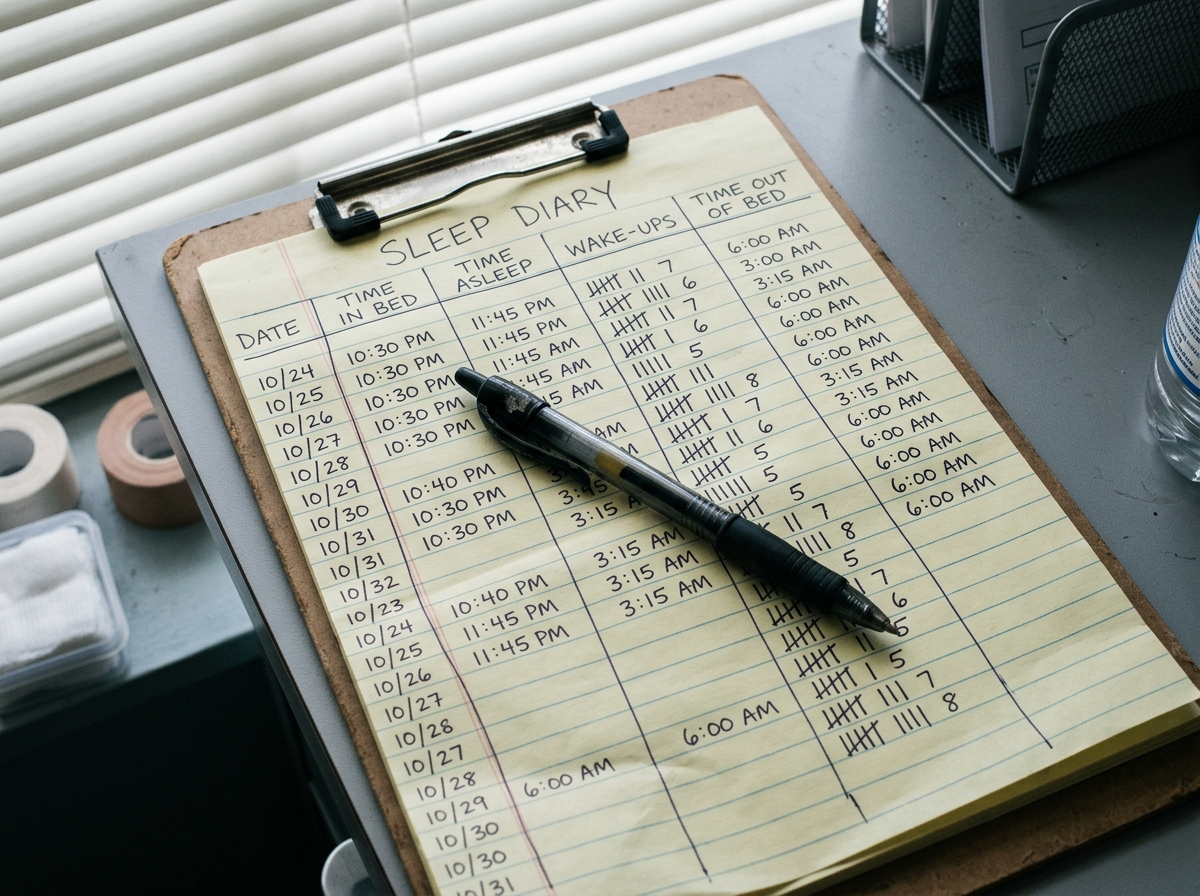
Donna spent two years on creams and over $400 before she reached my table.
By week two on the right bottle she had a sheet back over her feet. The first sensory change started inside the first week: the burning backed off enough that she stopped standing at the sink at two in the morning every night. By month two she was walking her dog the old two miles.
This is not magic and it is not fast for everyone. About one in eight people in the trial records I reviewed saw nothing. I'm going to tell you exactly what I found, in the order I found it.
My name is Dr. Renee Calloway. For seventeen years I have been a podiatric physician in a strip-mall clinic outside Cincinnati.
The patients who stay with me longest are the ones whose feet are on fire, and by the time they reach me, most have stopped believing anyone can help.
What Every Burning-Feet Patient Describes Before She Sits Down
The burning almost always starts the second they lie down.
Once the house is quiet there is nothing left to distract from it, and the feet take over.
I hear the same details on a loop.
They sleep with their feet outside the covers. They press one foot hard on top of the other at three in the morning for a few seconds of quiet.
If you are reading this, you may recognize your own night:
- Burning or stabbing the moment you lie down
- Electric jolts that snap up through the toes
- Skin so raw a sock or a sheet is unbearable
- Feet hanging off the end of the bed for relief
- Standing at the sink at two in the morning running cold water over them
- Being told it is circulation, or aging, and handed a cream
Three or more of these, and you are not at the start of this. You are well into it.
The cost I watch most often is not in the feet.
It is the marriage that quietly reorganizes itself around a pain no one else can see.
$400 In A Drawer. Every Tube Aimed At The Wrong Layer.
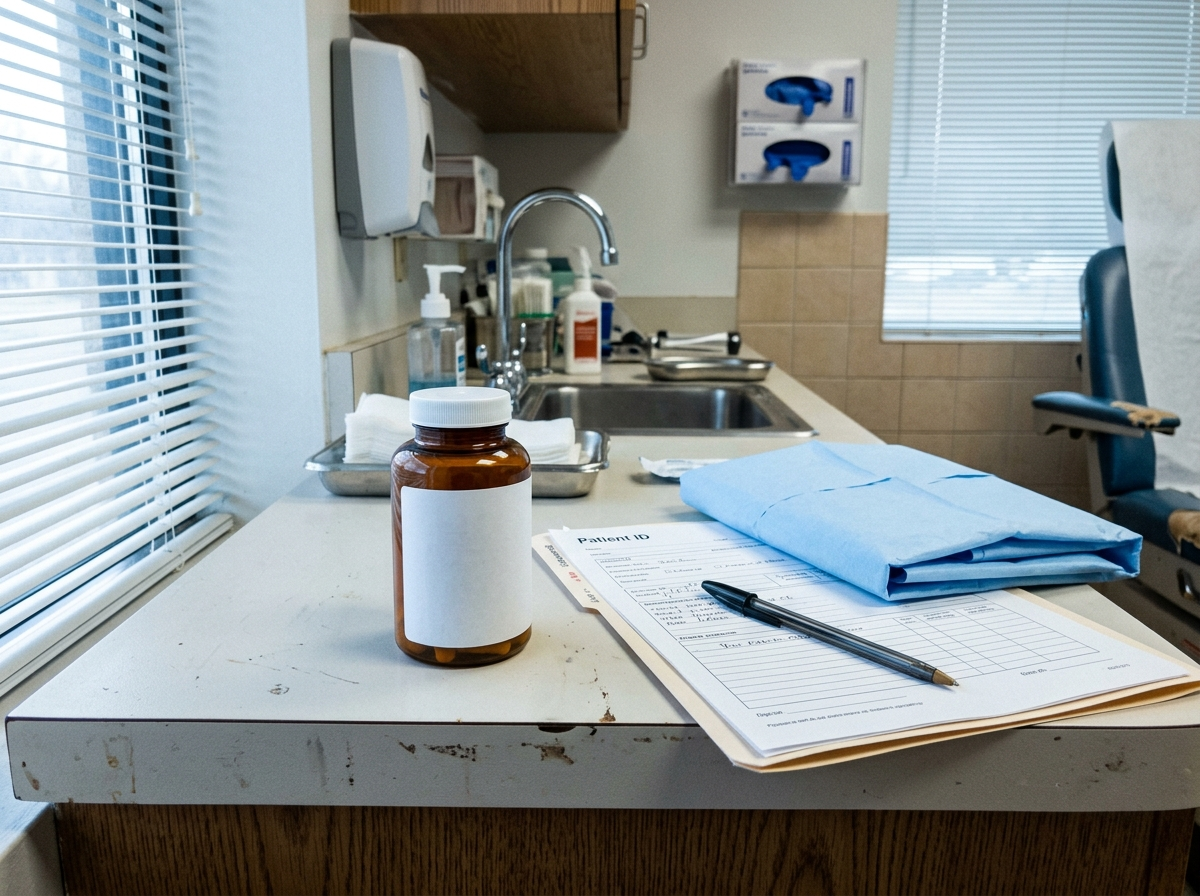
By the time someone reaches me, the bag is always full of the same things.
Lidocaine. Capsaicin (which more than one patient has described as setting their feet on fire to treat a fire). Menthol gels. Cooling sprays. A foot bath used twice.
Every one was prescribed by someone the patient trusted.
And every one of them was aimed at the surface of the skin, which is not where the problem lives.
I called a referring physician once about a retired electrician named Frank who had been burning for two years. The chart note read, in full: "peripheral neuropathy, advised OTC lidocaine, reassured."
I asked whether anyone had looked at what was driving the burning. He said, and I wrote it down:
"At his age, Renee, you manage it. You don't fix it."
That sentence is the whole problem in five words. Manage it, don't fix it.
Creams and gels: one to two hundred dollars. Cooling socks, braces, foot baths: another hundred. Two to four office visits to be told the same thing.
The average lands north of four hundred dollars, and not one of them was ever given a reason their feet were on fire.
I don't blame the patients for a dollar of it. I blame the reflex that treats a burning nerve as a dry heel.

A woman named Carol finally made the pattern impossible to ignore. She emptied her bag of creams onto my exam paper one tube at a time, the way you would lay out evidence.
She wasn't angry. She was finished hoping.
I had spent years being one more stop on a tour of people who couldn't tell her why her own feet were on fire.
I went home that night and decided I was done managing it.
I wanted to know what was actually burning.
Five Months Of Reading And A $3,000 Conference: The Question I'd Been Asking Wrong
I am a clinician, not a true believer in anything.
So I spent five months reading the neurology, calling two researchers, and paying almost three thousand dollars to attend a pain-medicine conference on my own dime.
What I found reorganized how I see every burning-feet patient on my table.
The fire was never coming from the skin we kept treating.
It was coming from one specific place none of those creams could reach.
I will not ask you to take my word for any of it. Before I tell you what I now hand my own patients, you need to understand where your feet are actually burning from.
Smoke vs. Wire: Why Every Cream In That Bag Was Aimed At The Wrong Layer
What I finally understood is something I can now explain to a patient in under a minute.
The burning is not coming from the skin.
It is coming from the small nerve fibers just beneath it, the ones that carry heat and pain.
In a neuropathic foot, those fibers misfire. They report a fire that is not there.
The skin those fibers sit under is, in the clinical sense, fine.
That is why looking at the foot tells you almost nothing, and why the entire shelf of creams is aimed at the wrong place.
Cream cools the skin.
The fire's in the wire underneath.
And PEA is the compound your body already makes to calm the wire.
That sentence is the whole correction.
A topical cools or numbs the surface it can touch.
The misfiring fiber sits below the depth it can reach.
No cream failed because it was weak. They failed because they were never near the problem.
PEA is not a drug I prescribe.
Your body already makes it to settle overactive nerve and immune signaling.
The supply runs short when the signaling stays switched on.
The form that reaches the fiber is micronized for absorption, given at the six hundred milligrams the published trials used.
So the question I had been asking my patients for years was the wrong one.
It was never which cream.
It was how to give the body more of what it uses to quiet the wire.
Why Nobody In The Cream Aisle Will Ever Name This. It Is Not A Conspiracy. It Is Worse.
I stopped being angry about this a while ago.
The cream aisle is not broken. It is working precisely as designed.
It treats the layer that is easy to sell to, then sells again when the layer underneath keeps firing.
A clinic visit ends in nine minutes with a sample tube because that is faster than explaining a nerve.
None of it was built to reach the wire, because reaching the wire would end the sale.
What I Now Hand The Patients Who Tried Everything
The compound I started recommending is a micronized PEA at six hundred milligrams.
The brand I settled on, after checking the third-party testing myself, is Youfirst.
Micronized matters because un-micronized PEA largely passes through unabsorbed.
Six hundred milligrams is the dose carried through the published trials.
Aggregate review of multiple clinical trials. Verified independently before launch.

Buyer check one: micronized, so the powder is milled fine enough to absorb instead of behaving like a generic shelf capsule.
Buyer check two: 600mg, the studied dose I want patients to recognize before they compare bottles.
Buyer check three: a 90-day money-back guarantee, because this is a weeks-long trial, not a one-night test.
I did not announce it to my patients as a breakthrough.
I am too old for that word.
I told the ones who had tried everything that there was something that worked on the right layer, that it was slow, and that I wanted to track it.
If you have already tried everything, the full formula and the dosing I use are at the link.
This is not a discount countdown. Micronized PEA has to be milled and tested in small runs, so Youfirst does not keep unlimited bottles sitting everywhere.
The current June batch is listed at 1,126 bottles. When a batch is gone, the next one is usually weeks behind it while it is milled, checked, and released.
Donna was one of the first I gave it to.
She came back at two weeks and told me, almost suspicious, that she had started sleeping with a sheet over her feet again.
Not every night.
But some, and for Donna, some was a number she had not seen in two years.
Across the patients I have tracked on it, the pattern is consistent and unspectacular, which is how I know it is real.
Most start near an eight out of ten on the burning.
By weeks six to eight, most report a three or a four.
Nightly wake-ups from the feet fall from five or six to one or two.
A portion feel little or nothing, and I tell them that before they begin.
By the second month, Donna was walking her dog again in the mornings.
Short loops at first, then her old two miles.
She told me she had stopped planning her evenings around how bad the night was going to be.

The woman who had laid four failed creams on my exam table and asked why no one ever told her why it was burning came back to tell me she had finally stopped thinking about her feet at all.
I want to be honest about the ceiling.
This does not cure neuropathy, and it does not reach everyone.
For most of the patients I see, it does the one thing the creams never could.
It reaches the wire and quiets it, slowly, the way the body would on its own if it could keep up.
What another year of this actually costs you.
- Sleep: five or six wake-ups a night becomes 1,800 to 2,100 broken moments a year, before you count the mornings you lose to the fog.
- Money: $400 in creams can become $600 to $1,200 a year once you add braces, foot baths, extra visits, and another tube someone told you to try.
- Health risk: living on pain relievers, sedating scripts, or stronger numbing options can create a separate long-term burden for the stomach, kidneys, balance, and clarity.
- Relationship cost: the bed becomes a place your spouse learns not to touch, move, or ask about, because the feet are running the night.
- Mechanism cost: the wire does not heal itself just because you learn to live around it.
One patient phrase has never left me. She said, "I waited six years before I tried this. I cannot get those six years back."
That is the sentence I think about when a patient tells me she is going to give the creams one more year.
I'm not going to tell you this is a miracle.
I have spent seventeen years watching miracles wear off by the follow-up appointment.
I will tell you what I tell the patients who have run out of other ideas.
The micronized Youfirst PEA at six hundred milligrams is what I now reach for first when someone's feet are burning and the creams have failed.
It works on the layer that is actually on fire, which is the one layer nothing in that bag of theirs ever reached.
It's $29.99 a bottle on the subscription, or $59.99 for buy two get one free.
Without the subscription it is $39.99 for one, or $79.99 for buy two get one free.
I tell patients to start on the subscription, because this works over weeks, and the people who stop at two weeks stop just before the part that matters.
I will give you the same caution I give them.
This is not fast, and it is not for everyone.
A portion of patients feel little, and I would rather you hear that from me than feel misled.
It does not cure the nerve. It quiets it.
I don't put my name behind anything I haven't watched work on my own patients.
And the company gives you ninety days.
If it does nothing, you return it inside that window and you are refunded, which is more than a nine-minute visit and a sample tube ever offered you.

If you do nothing, nothing changes.
The burning will be there tonight, and the creams in the drawer will still be aimed at the wrong layer.
That is not a scare line. It is just the trajectory you are already on.
This is the formula and the dosing I use with my own patients. Read it for yourself.
Youfirst PEA 600MG Micronized
- Subscription: one bottle for $29.99
- Subscription: Buy 2 Get 1 Free for $59.99
- One-time: one bottle for $39.99
- One-time: Buy 2 Get 1 Free for $79.99
90-day money-back guarantee. Return it inside the window for a refund.



Cheap PEA bottles can look similar at a glance. The two details I check are the same two I teach patients to check: micronized form and 600mg dose.
If the current Youfirst batch is gone, I would rather see someone wait than buy a lower-dose, non-micronized bottle and decide the whole compound failed.
P.S.
Donna still comes in once a year.
Last visit she spent the first two minutes telling me about her granddaughter and never once mentioned her feet.
For seventeen years, feet were the only reason anyone sat in that chair.
She had simply forgotten to bring hers up.
That is the whole job, right there.
If you check the page and the current batch is gone, the practical reason is usually milling and testing, not a marketing timer.
Comments
My podiatrist mentioned this.
I have tried everything.
Does it really work, or is it another one that quits after two weeks?
Week 7 for me.
I went from waking up five or six times a night to once, maybe.
The burning is a 3 now instead of an 8.
Slow, but it is real.
Everything "works" until it doesn't. What happens when you stop taking it?
Replying to Ed: I ran out for ten days and the burning started creeping back, so I just stay on it. Five months in now, still good on the nights I take it.
My wife is a retired nurse and knew every reason to be skeptical.
She is the one who told me to stop arguing and take it.
Eight weeks, and I sleep with the blanket on my feet now.
Three weeks.
Walked the dog this morning without thinking about my feet once.
I had forgotten what that was like.