AN ENDOCRINOLOGIST'S NOTE
“She Did Everything I Asked. Her A1C Was 5.7. Her Feet Burned Anyway. Here Is What 12 Years of Endocrinology Did Not Teach Me to Look For.”
I told her the burning often eases as the numbers hold. She trusted me. Six months later her A1C was still in target and she was sleeping on the couch. The trial I read after that visit told me why.
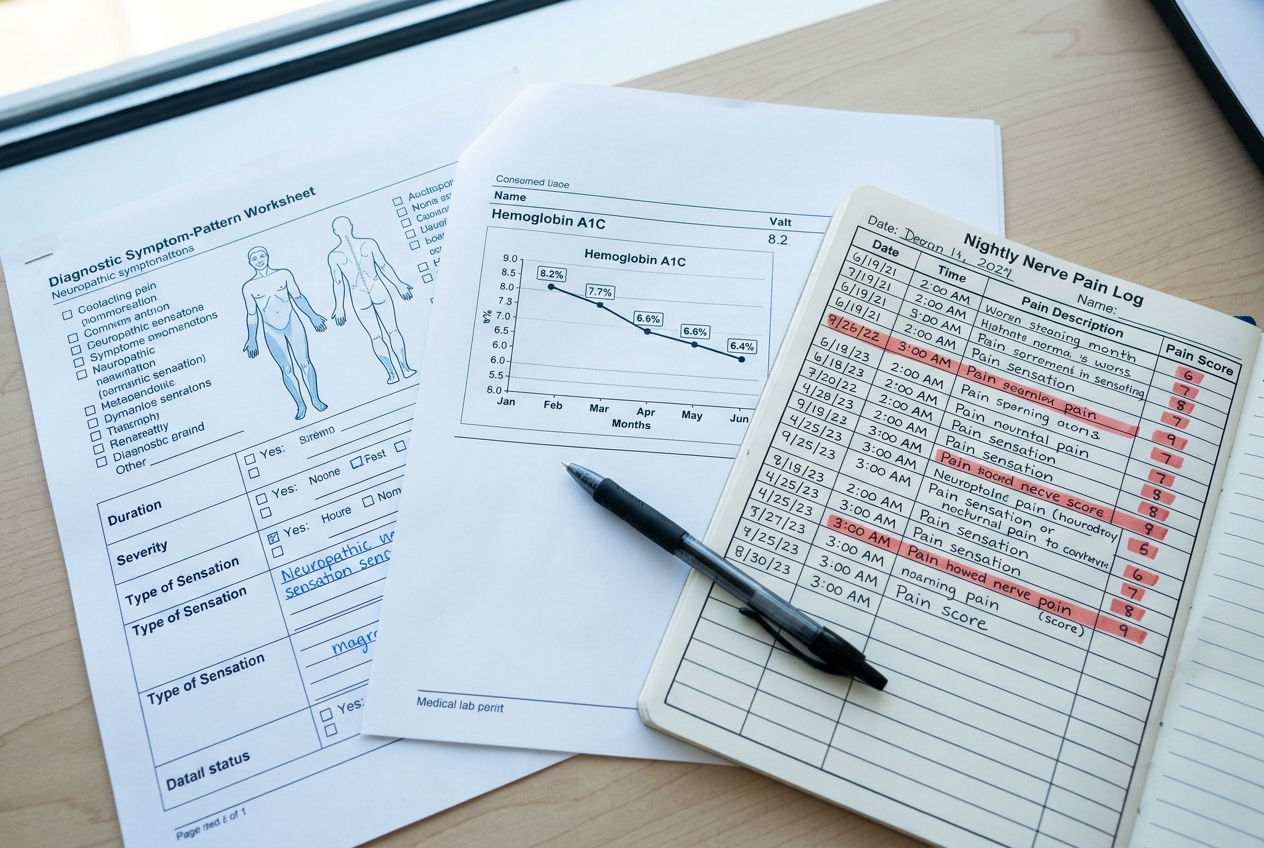
I will call her Donna. She is sixty-two, type 2 diabetic for nine years, A1C down from a 7.9 to a 5.7, weight off, blood pressure in line.
By every metric on her chart, she was the patient endocrinology is built to celebrate.
She told me, in eight minutes, that she had not slept in her own bed in fourteen weeks.
She slept on the couch because her feet burned through the sheets. She kept the tap running cold over them at 2 a.m. so the rest of the house could sleep.
I did what I had been trained to do. I congratulated her on the A1C. I told her the burning often eases as the numbers hold. I wrote her a gabapentin script for the nights and asked about her next bloodwork.
I was wrong about every part of that visit except the A1C.
The compound that turned out to matter is one the body already makes. It is called PEA, palmitoylethanolamide. In a nerve that has run under chronic diabetic strain, the supply runs out long before the numbers come back into line.
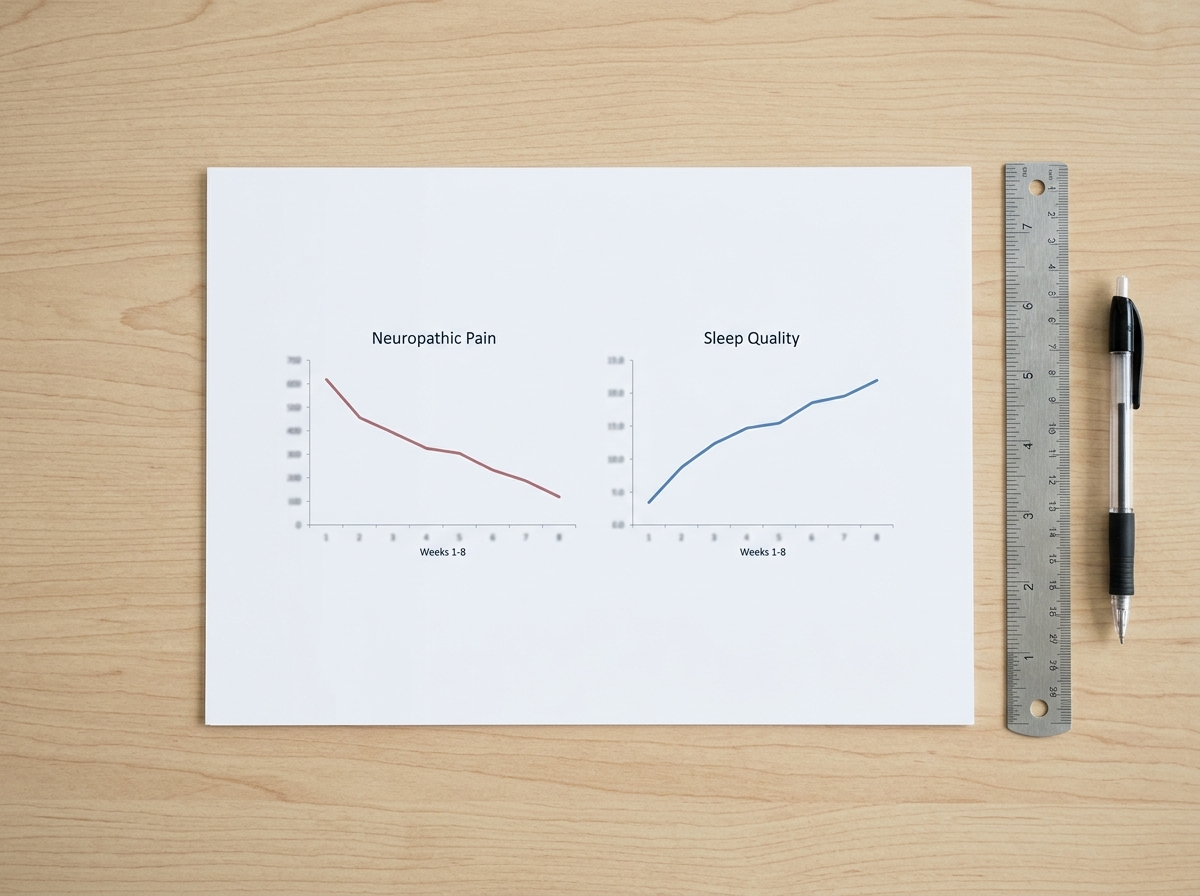
By eight weeks, patients given 600 milligrams a day had lower diabetic nerve pain while blood sugar stayed controlled. In early symptom logs, the first sensory shift sometimes started inside the first week: the sheets felt less hostile and the midnight burning stopped forcing the cold-tap ritual as often. Sleep improved after that.
This is not magic, and it is not fast for everyone. About 1 in 8 people in the wider evidence set still saw nothing.
I'm going to show you exactly what I found, in the order I found it.
Aggregate read of PEA neuropathic-pain trials and pre-launch clinical review. Verified independently before launch.
The 8-Minute Appointment I'll Spend the Rest of My Career Apologizing For
Donna came back in late spring. The A1C was still 5.7.
She had not slept in our bed in six months.
She had tried what the cabinet sells. Lidocaine cream that numbed the top of her skin and reached nothing under it. Cooling spray. Diabetic socks her feet could not tolerate. Alpha lipoic acid for three months because a forum told her to give it time.
She had given it time.
The gabapentin let her sleep through the worst of it. It did nothing to the daytime burning, and she had stopped asking why.
That is the part I want every clinician reading this to sit with for a moment. She had stopped asking. Because the last person she asked had told her the numbers were what mattered, and the numbers were excellent.
I went back to her chart that night. Then I went back to the chart of the patient before her, and the one before that.
Across the last twelve months of my clinic I counted thirty-six patients with diabetic peripheral neuropathy and an A1C at or under 6.5.
Twenty-nine of them had told me, at some visit, that the burning was unchanged or worse.
I had written some version of “it often eases as the numbers hold” in twenty-one of those notes.
A patient whose numbers look excellent can be counted as a success while she lies awake every night.
I had been counting them.
Why Every “Failed Patient” in My Practice Tells Me the Same Story
Once I started asking, the pattern was almost monotonous.
A1C dragged out of the sevens and into target. Weight down. Burning unchanged.
The shelf of failed solutions in her bathroom was usually the same shelf. Numbing cream that ran out and got refilled. Soaks. A heating pad that the burning made unbearable. Two or three supplements a forum had promised, mostly used, the receipts in a drawer.
Each one targeted the surface of the symptom. None of them touched what was driving it underneath.
The standard next step at this point is gabapentin or pregabalin, and I had written my share. They work by turning down the volume of the nerve's pain transmission.
They do not ask why the signal is screaming in the first place.
This is the structural point worth stating plainly.
The metabolic model treats a falling A1C as a treated patient. It was never designed to measure whether the nerves themselves have stopped firing.
Patients like Donna were not failing the model.
They were the patients the model is built to record as a success.
The Compound the Body Already Makes. And Why Diabetic Nerves Run Out of It.
The compound that kept coming up in the diabetic-pain literature is one the body produces on its own.
PEA, palmitoylethanolamide, is a fatty-acid amide the body makes on demand at sites of inflammation. Its job is to calm overactive immune and nerve signaling before it runs away from itself.
In a diabetic nerve under years of strain, that on-demand supply appears to fall behind the demand.
Mast cells stay activated.
Glial cells stay amplified, and the nerve keeps firing pain signals long after the original metabolic insult has been brought back under control.
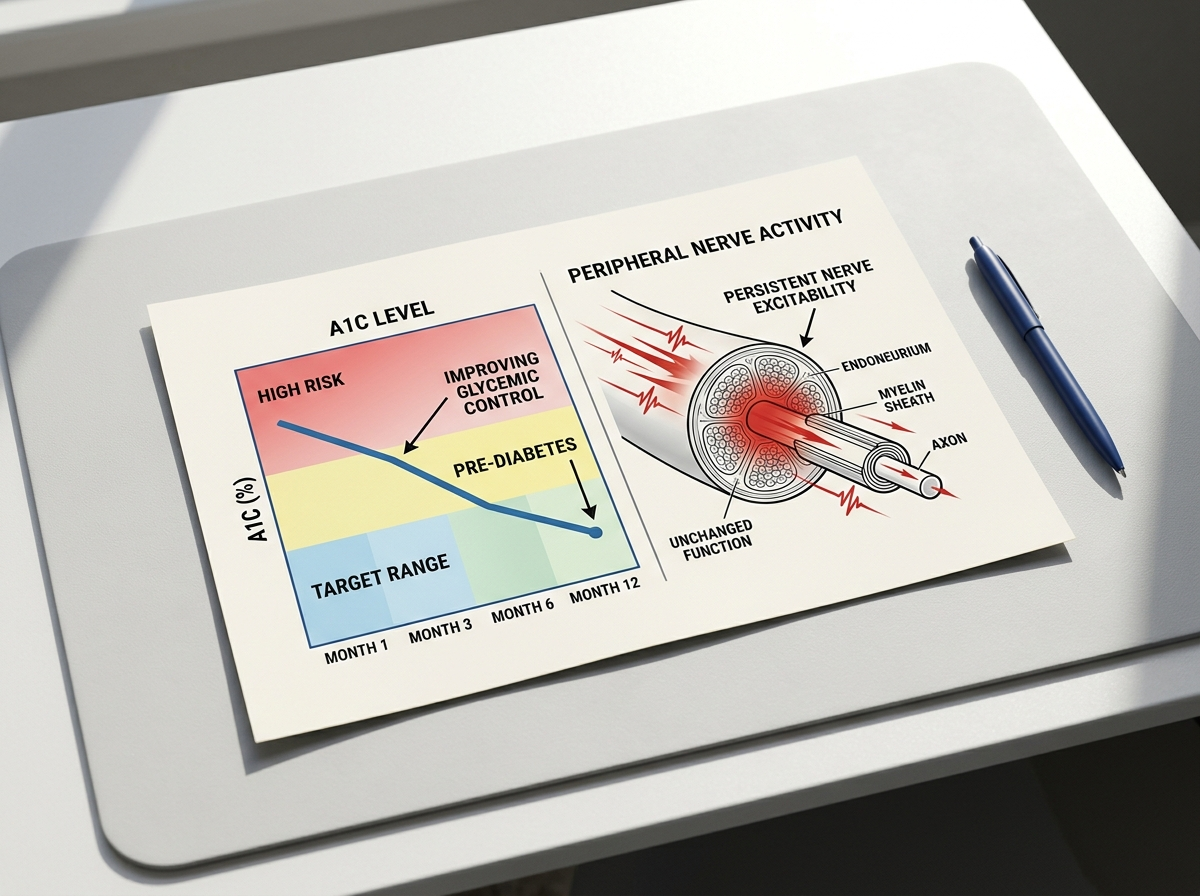
This is where the gap between the chart and the patient's nights becomes legible.
Controlling blood sugar stops adding fuel to the fire.
It does nothing for the nerves that are already on fire.
Calming that over-firing is a separate job. It is the one I had never been asked to do, because the metric I had been trained to chase did not measure it.
The clearest way I have found to explain it to a patient is a gas leak.
Shutting off the gas line is necessary. It stops the supply.
It does nothing for the flames already burning in the room.
The mechanism that quiets those flames runs through PPAR-alpha, the down-modulation of overactive mast cells, and the calming of glial amplification.
None of those routes depend on blood sugar. They explain, for the first time in a way I found clinically usable, why a patient with a 5.7 A1C can still be burning at 2 a.m.
A model that measures only the fuel will keep calling a patient treated while the fire she is describing goes unaddressed.
The Trial That Made Me Change How I Treat My Diabetic Patients
What changed my practice was not the mechanism on paper. Plausibility is a reason to look. It is not a reason to act.
What changed my practice was a controlled trial.
A randomized study in patients with diabetic neuropathic pain gave 600 milligrams of PEA daily for eight weeks. Seventy patients. The pain came down in a way the placebo arm did not. Sleep improved.
The line that mattered to me, the one I underlined twice, was the one I had spent twelve years assuming impossible.
The pain fell while blood sugar was held constant.
Something other than glucose control did the work.
I will report this with its limits, because evidence without its limits is marketing.
One direct diabetic-neuropathy trial is not the whole literature. Seventy diabetic patients across eight weeks is a signal, not a closed verdict. It asks for replication. It does not grant certainty.
It is, on the other hand, the most direct evidence I have ever read for the specific patient I had been failing.
And it is the only compound I have come across that addresses the mechanism the metabolic model cannot reach.
The single most relevant detail is the simplest one.
In that trial the pain fell while blood sugar stayed exactly where it was.

What I Now Tell Patients With a 5.7 A1C and Feet That Still Burn at Night
The first thing I tell them is the part I should have told Donna at the first visit.
Your numbers are not the reason the burning will not stop. The burning is inflammatory nerve over-firing that the metric we use to grade your diabetes was never built to measure.
The second thing I tell them is which patients the evidence above is most likely to apply to. The pattern is narrow and specific. If most of the following describe you, you are, on the trial above, the exact patient the standard care plan is built to record as treated while leaving you burning.
- Your A1C is at or near target.
- The burning is worse at night than during the day.
- You cannot tolerate socks or a bedsheet on your feet.
- Gabapentin helps you sleep, but the daytime burning continues.
- Months of good numbers have not changed the burning.
The third thing I tell them is what to look for if they want to evaluate PEA themselves.
The dose has to match the trial. Six hundred milligrams a day. Not the under-dosed amounts common on the category shelf.
And the form has to match the absorption problem.
PEA is poorly soluble. Grinding the particles smaller, what the literature calls micronization, raises the share the body can take up.
That is the difference between a dose printed on a label and a dose delivered to the nerve.
The formula that meets both criteria, and the one I have seen patients return to after the cabinet of failed creams, is Youfirst PEA 600MG, micronized.

The buyer's check is not complicated.
Micronized, so the form is built for absorption. 600mg, because that is the studied daily amount.
Neither detail is hype. They are the minimum facts a serious PEA bottle should be able to show.
What distinguishes it is narrow and factual. It matches the only dose the evidence actually supports, in a form built to be absorbed.
The verdict is measured.
The evidence does not show a cure, and I do not claim one.
What it shows is a compound that addresses the mechanism glucose control cannot reach, at a dose with trial support, in a form designed for absorption.
For the patient I described in my opening, that is the most direct match between her problem and an option I had not been trained to put on her table.
What another year of this actually costs you.
- 1,400 to 1,900 broken sleep hours: 4.2 hours of fragmented sleep a night becomes a year of mornings that start already damaged.
- $480 to $1,900 in repeat spending: creams, diabetic socks, refills, supplements, co-pays, and one more bottle from the cabinet of things that almost made sense.
- 2 or 3 half-asleep walks across a dark room each night: after 60, numb feet plus poor sleep is not just discomfort. It is a fall-risk pattern.
- 180 more nights on the couch: the bed becomes something your spouse sleeps in while you keep the tap running cold at 2 a.m.
- 365 more days of an untreated signal: a good A1C can stop feeding the fire, but an over-firing nerve does not become quiet just because the chart looks clean.
I am forty-eight. The patient who left this in my intake comments is seventy-one.
She wrote, "I waited eleven years before I tried this. I cannot get those eleven years back."
That is the line I read on the worst night I had with Donna's chart, and it is the line I want you to read before you treat another year of burning as a normal number on a lab report.
For readers who want to evaluate the formula themselves, the full label, the 600-milligram dosing, and the trial behind it are available at the link below, along with the manufacturer's terms.
The product carries a 90-day money-back guarantee, stated by the manufacturer as a full refund within that window if the result does not hold.
I take no commercial position on the purchase. I am reporting what I now tell the patients I had been failing.
The dose matches the evidence. The form addresses the absorption problem. The mechanism is the one the metabolic model does not treat.

Per the manufacturer's stated terms.
The full formula and the trial behind it are at the link below.
Current batch note: 1,743 bottles remaining at the time of this writing.
See the formula and the trial behind it →90-day money-back guarantee, per the manufacturer's stated terms.
P.S.
The detail worth keeping is the one I had spent twelve years assuming impossible.
The pain eased while blood sugar stayed exactly where it was.
A good number was never going to be the thing that put the burning out, and there is now at least one documented reason why.
If you have been told yours would, and it has not, this is the question I would now ask in the visit I should have asked it in.
Supply note: if this batch sells through, the next run can be delayed for weeks while the micronized powder is milled and tested.